
The One Hormone Nobody Mentioned At Your Appointment
Your doctor was right. It is hormonal. Here’s what she left out.

Women kept asking me about their hair toward the end of their appointment. I could tell them exactly what was happening. Then they would ask what to take, and I had nothing.
I had read the labels. One ingredient on its own, at a dose nobody would print. Blends that listed everything and measured nothing.
I was not going to hand that to a patient and tell her it would help.
So I made the one I would hand her.
I’ve spent over twenty years treating hormonal systems. Perimenopause hits them harder than almost anything else your body goes through, and your hair is usually where you notice it first.
The women who came to me about their hair kept saying the same thing. Not about the hair. About whether anyone believed them.
It usually came out like this:
“Dr. Barron, I can see my scalp now. Everyone keeps telling me it’s just my age and there’s nothing to do. I’m not imagining this, am I?” A patient, 51 · a version of this I hear every week
She wasn’t imagining it.
She had been given pieces of it. Never the whole thing. By the time a woman sits in my office, she’s usually heard every one of these sentences, in roughly this order:
“It’s just hormones.”
“It’s just aging.”
“Your labs are all normal.”
“It’s for life now.”
Read them again. None of them are wrong.
Estrogen is a hormone. Aging is real.
Her labs really can come back normal while the part keeps widening. Every one of those is true. And every one of them leaves out the most important part.
A patient of mine sat in her car in the parking garage after a dermatology appointment and cried. She told me about it months later like it was something she should have been embarrassed by.
The dermatologist had not been unkind. She looked at her scalp and agreed she was losing hair.
Then my patient told her she was already taking the vitamins and using the five percent minoxidil, and the dermatologist told her that was about all there was.
Eleven minutes. Back in the elevator with nothing she didn’t walk in with.
That is not one bad doctor. She was telling my patient what she had been taught. Researchers asked medical residents how prepared they felt to manage menopause. Twelve out of a hundred and seventy-seven said they were ready.
She got four true sentences and never the fifth. Almost every woman I see gets the same four.
There is one part I never had to explain to a single one of my patients.
You already know the exact spot in your bathroom where the light is worst.

That’s where you check. You lean over the sink and lift your part with two fingers to see if it’s wider than last month.
Some mornings you angle your phone above your crown for a photo. Then you wish you hadn’t taken it.
You run a hand through and count what comes out. Ten strands, twelve, sometimes even more.
The ponytail you used to fall back on is half of what it was. You swear the elastic goes around one more time than it did.
And the hair itself doesn’t feel like yours anymore. Finer. Drier. It will not hold a style. You’ve caught yourself thinking, whose hair is this.
And it costs you time you never used to spend. An hour dyeing it every month, because the grey shows first at your temples, where there is least hair to hide it. A morning that takes twice as long as it did. None of it to look good. All of it to look normal.
Somewhere in there you stopped wearing it down. You know which rooms in your own house to avoid, and which chair at the table. You got quick at saying no to the group photo.
A patient told me she had started wearing bigger earrings. Not because she liked them. Because it cut down on being called sir, and it mostly works. But not always.
Estrogen Was Protecting Your Hair. Then Your Estrogen Declined.
This is the fifth sentence. Nobody said it to her, and nobody said it to you.
I draw it for them. Same drawing every time, on the back of whatever is sitting on the desk.
You already know estrogen drops. Everyone knows that part.
Here’s the part that gets left out. Estrogen wasn’t only running your cycle and your temperature. It was also protecting your hair, holding each follicle in its growth phase longer than it would have stayed on its own.
Then it falls. And your follicles lose it.
“So what takes over?” one patient asked me. She had her pen out by then.
Androgens. One in particular, a hormone called DHT. She wrote it down and asked me to spell it.
It is not new and it is not obscure. It had never come up in a single appointment she had already been to about her hair.
It was always there. Estrogen was just keeping it off your scalp.
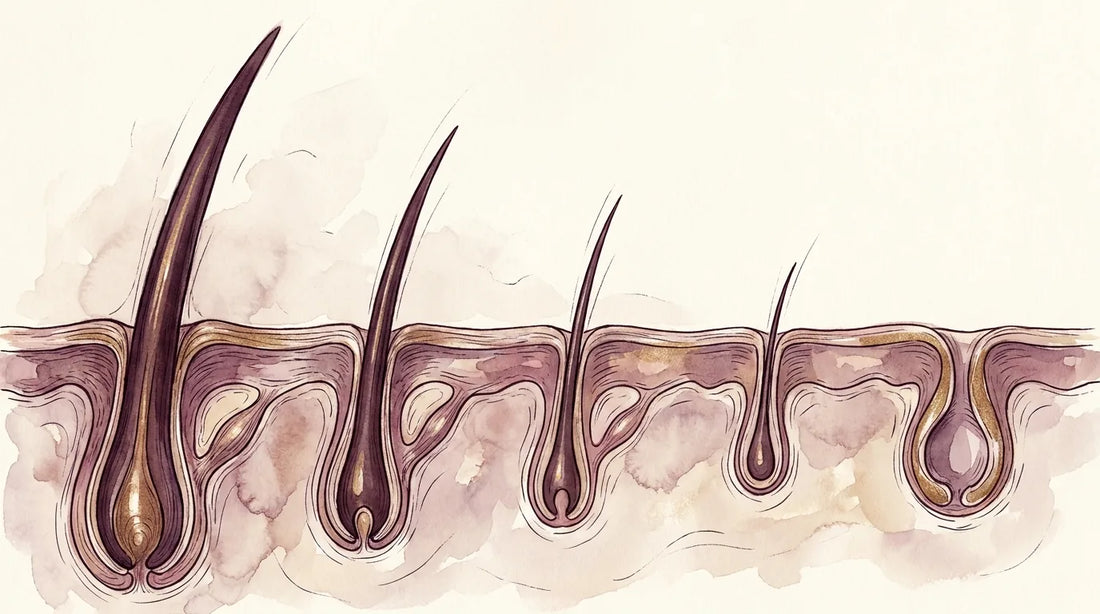
DHT shrinks the follicle a little more each cycle. The strand grows back a little finer. Then finer again.
Estrogen was doing one more job, and it is on the same drawing.
Your scalp is skin. Same as your face. Estrogen held that layer up too. When it goes, that layer thins too.
You already know this about your face. It is what every ad about firmness has been telling you for ten years. Nobody ever applies it upward.
You have a whole shelf for the skin on your face. You have never once looked at the skin your hair grows out of.
I use a plant when I explain it. You can water the leaves all you like. If the soil has thinned out, it comes back smaller every season.
A hair does not grow out of nothing. It grows out of that layer. The layer thins, the follicle loses its footing, and the strand it makes comes in finer.
So you have been treating the hair, and not the ground it grows out of.
That’s what’s happening in your bathroom. The same number of follicles you have always had. Each one a little smaller than last year. That’s why the part looks wider in the overhead light.
By then I have usually put the pen down.
It’s thinning strand by strand, from the inside, which is why you never see it come out in clumps.
The strands on the brush. The drain after a wash. The photo someone else took, where you only look at your own hairline.
One change sits behind all three. The estrogen that was protecting those follicles is gone.
“It’s just hormones.” That sentence is true. It’s also unfinished.
Here’s the rest: it’s a specific hormone shift, with a specific mechanism behind it. And “just aging” is unfinished the same way.
Aging is the trigger. The mechanism underneath it is the part you can actually work on.
Estrogen swings, then trends down. Your follicles start losing their protection years before your last period.
Estrogen settles low. DHT pressure on each follicle now runs unopposed.
Estrogen stays low. The protection doesn’t come back, and the collagen doesn’t rebuild on its own.
The three differ in how far the estrogen has dropped. What is happening underneath is the same in all of them.
52.2% of postmenopausal women have female-pattern hair thinning.
In a poll of roughly 6,000 women, about 1 in 2 noticed it during the transition itself.
It’s that common, and almost nobody is told.
Menopause (journal), 2022. Newson poll. See references.
4.9 · 1,135+ reviews
The formula I built to work on it
One dose a day. Eleven actives, every dose on the label.
Shop The FormulaThis One Doesn’t Wait Itself Out
Unlike the shed some women get after a baby, perimenopausal thinning doesn’t resolve on its own.
Every cycle that passes, a few more follicles shrink. A follicle that shrinks long enough eventually quits.
You can’t rush hormones. But every month you wait gives it more time.
Another had been told twice she was too young for this. She was forty-four. You hear that from a doctor and you go home and believe it. She lost two years that way. “She never said the word perimenopause,” she told me. “Not once.”
So I tell them what they can do.
You can do something about the follicle that lost its protection, and the ground it grows out of.
For years the advice was to grab a single hair vitamin and wait.
But the studies that held up over time tested combinations of ingredients, never one ingredient alone.
The follicle changed and the ground changed. One ingredient was never going to reach both.
Why What You Already Tried Didn’t Work
It usually sounds like this.
“I tried the biotin gummies. Then a collagen powder in my coffee every morning. Then saw palmetto capsules. Then a keratin supplement. Then the rosemary oil half of TikTok swears by. Then castor oil before bed, on an old towel so it wouldn’t wreck the pillowcase. One at a time, over about two years. Nothing changed.”
Of course it looked that way.
And by the time a woman says that out loud to me, she has usually started reading about minoxidil, and spironolactone, and the injections where they spin your own blood and put it back. She has looked up what a transplant costs and closed the tab when she saw the price of a single session.
One woman said it plainer than I would have. She said she finally understood why people freak out and run off to Turkey.
Add up what your drawer cost. Two years of that, and nothing to show for it.
Your follicles lost their protection and the collagen thinned at the same time. Each supplement on its own touched one piece of one of them.
A drugstore biotin gummy was built for a twenty-five-year-old’s hair. It was never built for a follicle under DHT pressure.
And most of them hid their amounts inside a “proprietary blend,” so you couldn’t even check.
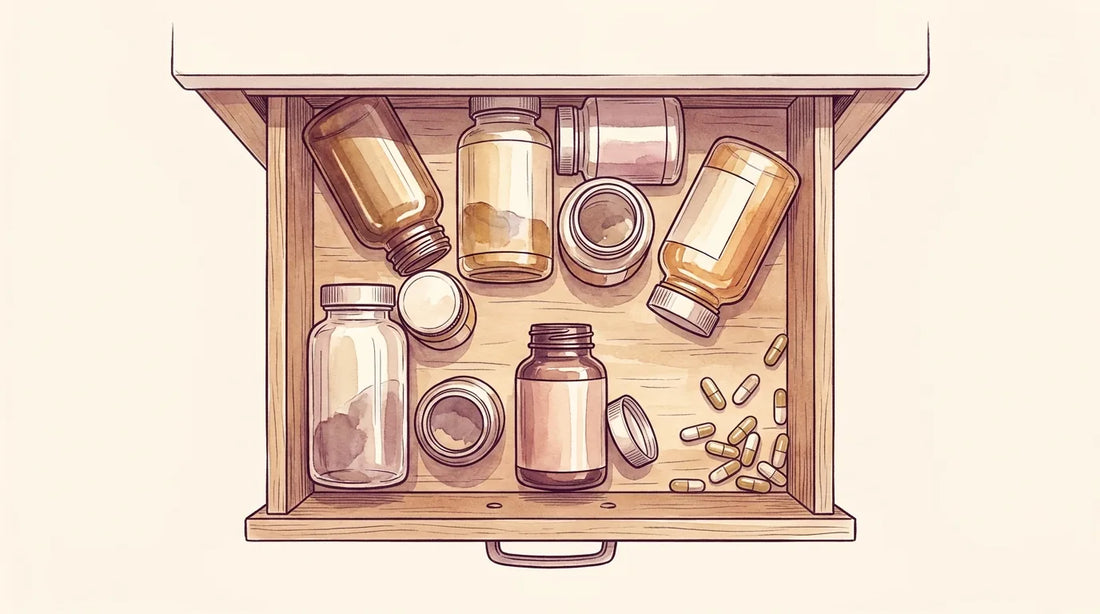
The drawer almost every woman brings me. Individual bottles, tried one at a time.
Why the drawer kept growing:
- A biotin-only gummy feeds the strand. That matters, but it does nothing for the follicle.
- A scalp serum works on the follicle. It does nothing for what the strand is built from.
- A thickening shampoo changes how hair looks for a day. It reaches neither.
A patient described the pattern to me once. A bad wash day sends you to Google. There is always another bottle, so you buy it, because buying it is the only thing you can actually do that day. Then she stopped and asked me something nobody had asked me before. “Am I just paying to feel like I am doing something?” I told her the truth. Most of the time, yes.
She was waiting for me to tell her she had wasted her money.
You weren’t failing at this. You were treating the strand and leaving the follicle alone, over and over, and nobody ever told you that is what was happening.
The formula was the problem. Not you.
Before you decide this is expensive, here is what the rest of it costs.
What trying everything costs
a drawer of single supplements, roughly $70 to $110 a month
add a subscription formula, roughly $70 to $90 a month
add PRP injections, commonly $1,000 to $2,500 a session
add a transplant, plus keeping all of it going
Ten thousand dollars and up over five years of trying everything, and every line of it has to be paid again the year after.
DR BARRON: from $29 a month, about $0.97 a day
Illustrative US prices, 2026. What any of this costs varies widely by provider and city, and none of these figures are quotes from us. Only the DR BARRON price is ours.
You have already been paying for this. Just not in a way that reached the follicle.
4.9 · 1,135+ reviews
From twenty-nine dollars a month
A full hair cycle is ninety days. That is exactly how long the money-back guarantee runs, so the risk is not yours.
Start the 90 daysFive Reasons I Built It This Way

If you’ve already spent real money on biotin, collagen, and whatever the last ad promised, you should be skeptical. I would be too.
After watching this play out in hundreds of women, I formulated what I wished I could hand them. It works on all three: the follicle, the ground it grows out of, and the strand itself.
Cancel anytime, and return it if nothing shifts.
What it does is support all three.
Take it alongside your HRT or your minoxidil.
1. It reaches the follicle, not just the strand.
What makes it different
Physician-formulated. Built by a board-certified endocrinologist.
Built for the mechanism. Every ingredient is in there for a specific job.
Every dose on the label. No proprietary blend, nothing hidden, a real list to take to your doctor.
Honest about the limits. It supports the pathways, and it works alongside HRT or minoxidil.
One daily dose. Built for a real life, not a six-bottle drawer.
For the follicle, under DHT: pumpkin seed and zinc.
For the ground it grows out of: collagen, vitamin C, silica and MSM.
For the strand itself: biotin, L-cysteine and selenium.
And vitamin D, because the follicle cycle depends on it.
2. It pairs ingredients the way the research tested them.
These work in pairs, not alone. Silica with biotin. Collagen with vitamin C. The research tested them together, so that is how they are dosed here.
3. Every dose is printed on the label.
 “Proprietary blend”Every dose printed
“Proprietary blend”Every dose printedOne patient printed the list and read every line of it before she ordered. She told me afterward that nobody had handed her something she was allowed to check before.
4. It holds up next to what you’ve already tried.
When a woman asks how this compares to what’s already in her drawer, I walk her through the same checklist I’d use for any plan.
How I’d judge any hair supplement, including mine
- Is every dose printed on the label, or hidden in a “proprietary blend”?
- Does it reach the follicle and the ground it grows out of, or only the strand?
- Can you check each ingredient against the published research?
- Did a physician formulate it, and is she honest about what it won’t do?
- Are the reviews and photos real, named customers?
Take this checklist to any brand. I built mine to pass it.
How it compares


A drugstore gummy reliably checks one box, the easy one.
None of those reach both. Ours pairs them the way the research tested them, in one dose you’ll still be taking in month three.
5. What I left out matters just as much.
The list is short on purpose.
Every ingredient had to have published research behind it. If it didn’t, it got cut, no matter how good it looks on a label.
4.9 · 1,135+ reviews
Eleven actives. Every dose on the label.
No proprietary blends. Nothing hidden behind a blend name, and every batch third-party tested.
See what’s in itWhat I tell my patients to expect
Month one is the foundation month. Most of what happens now happens underneath, though shedding is usually the first thing to change.
Then I give every patient the same instruction: pick one measure and check it monthly.
The elastic count, or a photo of the same part line in the same light.
One measure, once a month, same light. That is the whole method.
This works over a full hair cycle, so once a month is the right rhythm.
Ninety days is the checkpoint, because that’s one full hair cycle.
What to Expect, Cycle by Cycle
Hair grows on a roughly 90-day cycle, so you have to think in months, not weeks.
Day one to ongoing
The foundation month
It starts working the day you start taking it. Hair builds from the root out, so this first month happens underneath, before the mirror catches up.
Support compounds
Sticking with it is the whole game here. The strands that were already on their way out finish falling, and what you’re feeding keeps building underneath.
A full hair cycle
What you fed in those first weeks is what’s reaching the surface now. Give the follicle more time.
The long game
The pressure doesn’t stop, so this is a daily habit, not a course you finish.
If your thinning is sudden, patchy, or rapid, see a clinician, because those patterns can point to something else.
The words change too. One set of sentences at the start, a different set a few months in.
What women say when it starts:
- ❌ I can’t pin back the fluff, can’t wear my hair down, can’t chop it all off and still resemble a female
- ❌ I miss when I would get up, brush my hair, throw some clothes on, and be ready for my day
- ❌ I have a whole crop of wiry greys at my temples now, and I slick them back with gel
- ❌ The amount of maintenance it takes to keep things at a mediocre level is ridiculous
- ❌ The drains are clogging 5x as fast as they used to, and my stylist confirmed I’m losing more hair than ever before
What women say a few months in:
- ✅ I stopped counting what comes out
- ✅ I wear it up
- ✅ I let someone take the photo
- ✅ I stopped moving my part around to cover things
- ✅ Getting ready takes as long as it used to
Those are the sentences I remember. The survey put numbers to them.
What our customers reported
Here is what they told us:*
- 94% reported less shedding within the first month
- 89% found the gummies easy to stick with as a daily habit
- 88% plan to reorder to keep seeing progress
- 92% said their hair looked fuller and thicker
*Based on customer feedback and post purchase survey. Individual results vary.
Every woman asks me the same follow-up, usually looking at the floor. “Do you have to keep taking it?” Yes. That is the one sentence they got right, and the only one they finished. The pressure on the follicle doesn’t stop, so you can’t stop either. I’d rather tell you that now than have you find out in month four.
What The Published Research Measured
Here’s the science the formula is built on. Some of it tested a single ingredient. The most important of it tested a pairing.
Bamboo silica with biotin, tested together rather than one at a time.
A 90-day randomized trial tested that exact pairing in 105 women, and measured a growth rate of 0.57 mm per day in the silica-and-biotin arm.
That’s the bar we set for ourselves.
Collagen with vitamin C, for the structure the strand is built from.
A 12-week randomized trial of hydrolysed collagen with vitamin C measured a 27.6% increase in hairs per unit area against placebo.
And pumpkin seed is for the follicle. The pumpkin seed research was conducted in men, so it is not a women’s result.
See references.
Real Customers, Photographed Months Apart
Individual results vary. Use the arrows or swipe.
 MONTH 1
MONTH 1 MONTH 3
MONTH 3“My hormonal hair loss seemed to get worse every month, and I was afraid it would never improve. Now I don’t panic every time I wash or brush my hair because the shedding has decreased so much. My hair looks fuller, and I’m seeing encouraging signs of regrowth.”
Katherine B. MONTH 1
MONTH 1 MONTH 4
MONTH 4“After trying product after product, I honestly didn’t expect DR BARRON to make such a difference. Four months later, my shedding has noticeably decreased, my scalp feels refreshed, and I can see little baby hairs growing in. My stylist even asked what I’d been using because my hair looked so much fuller.”
Brenda B.Taking DR BARRON for 4 months MONTH 1
MONTH 1 MONTH 3
MONTH 3“My hair was thinning badly, and I hated looking in the mirror. Three months in, and my hair looks fuller and healthier.”
Marissa F.Taking DR BARRON for 3 months MONTH 1
MONTH 1 MONTH 3
MONTH 3“I was seriously considering medication after my hair kept getting thinner, but I decided to commit to this routine first. A few months later, I could already see a noticeable improvement. My hair feels stronger, looks fuller, and I’m finally feeling optimistic again.”
Carrie A. MONTH 1
MONTH 1 MONTH 3
MONTH 3“I originally bought it hoping it would help with my hair, but I ended up noticing more than I expected. After a couple of months, my hair felt healthier and the shedding had slowed down. By the third month, I could see tiny new hairs filling in around my hairline. It’s become part of my daily routine, and I don’t see myself stopping.”
Paula T.Real DR BARRON customers, uncompensated. Individual results vary.
More customer photos are on the product page.
Give it one full cycle.
From $29 a month on the 90-day supply, or $33 monthly. Free shipping on subscriptions, and free guides sent the moment you order.
 Shop The Formula
Shop The Formula
Questions Women Ask Me
No. And I would not trust anyone who tells you it will.
Nothing you swallow brings back what is already gone. What it can do is work on the hair you still have. That is the part that is still yours to keep.
Yes. It is built to sit alongside them, not replace them.
Talk to your provider before adding anything new.
Yes. High-dose biotin can throw off common blood tests, including thyroid panels. The result comes back wrong even though nothing has changed in your body.
Pause the gummies a few days before lab work and mention it to your doctor.
A lot of women come to me weighing the bigger options and not loving any of them. You’re tired of the idea of a drug you might be on for good. A transplant feels like a big, expensive step you’re not ready for.
You don’t have to make that decision to start doing something. That’s exactly what I built this for. One daily dose, no prescription.
Any real answer takes months.
Less shedding usually shows up before that. Fullness is what takes the full cycle.
That’s exactly why starting now matters: what you start today is what shows up next cycle. Waiting six months doesn’t pause the shrinking.
The 90-day money-back guarantee is built around one full cycle. If nothing shifts by the end of it, you get your money back.
No. Biotin is one of eleven actives.
If biotin alone were the answer, you wouldn’t be reading this.
Eleven ingredients, each one in there for a specific job, in one dose.
As for the price, this is that whole drawer combined into one bottle.
Bought separately, a collagen, a biotin, a pumpkin seed, and a mineral complex cost more per month, often several times more.
Perimenopausal thinning comes on slowly.
It spreads across the top and crown, not in patches, as estrogen falls.
If yours came on suddenly, shows up in patches, or comes with fatigue or other changes that don’t fit that picture, get bloodwork first so you’re addressing the real cause.
This formula works on the follicle, the ground it grows out of, and the strand itself.
It’s not a stand-in for anything your labs might call for.
You can do both.
Who It's For, and Who It Isn't
I won’t oversell this, because I don’t trust anyone who makes big promises about hormonal hair.
It works best for the woman who understands that this takes consistency, not a quick fix.
Who it's for
- Your part has widened, or the ponytail has thinned, since your cycles started changing.
- Somebody told you “it’s just hormones” or “it’s just aging,” and left it there.
- You have a drawer of single supplements that each did nothing you could see.
- You are on HRT, or minoxidil, or neither, and you want something that works alongside it.
Who it's not for
- Expecting visible results in a week or two.
- Sudden or patchy shedding (see a doctor first).
- Unwilling to take it daily for three months.
- Waiting because you think a topper or a part-spray will cover it.
- Looking for something that replaces a prescription.
- Currently being worked up for a thyroid or cardiac condition, until you’ve spoken to the clinician ordering your labs.
If the first list sounds like you, this is the formula I built for you. Start the 90 days.
The guarantee is there so you’re not risking anything.
It’s almost never just about the hair. There is a moment someone else notices, and you never forget it.
Maybe it was a friend’s little girl looking up and asking where your hair went. You brushed it off with “some women my age get this,” and tried not to cry in front of everyone.
Maybe it was a photo someone took from above, the angle you never see yourself from, and how much scalp was in it.
Maybe it was your hairdresser going quiet at the crown, where she used to chat.
Your hair was the part of you that still felt young. Still felt like you. You never say that part out loud.
About 1 in 2 women notice hair thinning in the menopause transition. You are not the exception.
It shows at the part and the crown first, before the hairline, which is why the overhead light gives it away before anyone else notices.
And it runs four to seven years on average, longer for some women, which is why what you do now matters more than any 30-day fix.
NAMS, Menopause 2020. See references.
I don’t remember the numbers. I remember the woman who was told there was nothing to do, and believed it for three years before anyone explained what was actually happening.
There is another side to this.
You wear it up without thinking about who is standing behind you. The weekend photos come back and you look at your face first, not the top of your head.
You stop bracing before the drain.
That’s what the women a few months in describe. They stopped checking, and they started feeling like themselves again.
A patient told me her camera roll used to be full of pictures of her own hair. Years of them. Then one night she deleted every one.
You really have two choices here.
A patient described getting ready to go out. Makeup done, curling iron, the whole thing. She caught the mirror on her way past the hall and stopped. She told me she almost didn’t go.
You can keep buying a new supplement every time a bad wash day scares you, trying one at a time and hoping you finally pick the right one.
Or you can try one formula built to reach all three, give it a full ninety days, and let the guarantee take the risk instead of you.
Either way, ninety days will tell you. You just have to start.
What Women Are Telling Me
From women who started a few months before you.
“I had my doubts thinking that this was another too good to be true product. But at the same time I’m very desperate to try and keep my hair. I’m 52 and going through perimenopause and my hair had been coming out in clumps. I didn’t notice any difference at first but after about 4 weeks I started to notice that the shedding wasn’t as bad.”
Felicia G.“Perimenopause made my hair thinner. I’ve been using the DR BARRON Gummies for 5 months now my hair is definitely feeling healthier and thicker.”
Diana M.“My doctor said it was hormonal and there wasn’t much I could do. A few months in, the shedding’s calmed down and my part isn’t as obvious.”
Hope B.“Since perimenopause my hair has felt thinner. I’m not sure if it’s my imagination or what, but shedding seems to have decreased.”
Cristina G.“I blamed everything but my hormones. I’ve been taking these for a few months now and I’m noticing way less hair in my brush.”
Suki E.“Nobody tells you your hair changes in your fifties the way it does. Feels like my hair has a little more life in it again.”
Sharon L.“My shedding has slowed down considerably, but not stopped. I’m going to keep going.”
Kimberly K.“My hair changed a lot in perimenopause. I was noticing thinning at my temples. PS my nails are so much stronger!”
Jill J.Real DR BARRON customers, uncompensated. Individual results vary.
From real DR BARRON members
Real customers who shared their photos. Individual results vary.









You Don’t Have to Just Watch It Widen
From $29/mo on the 90-day supply, about $0.97/day.
Shop The FormulaYou’ve been burned before, and that’s fair. Keep your skepticism.
94% of the women in that survey reported less shedding in the first month.
So the terms are simple: take it for the full cycle.
If you don’t feel the difference, you get your money back. Not store credit. Not a form that hopes you give up.

P.S. A follicle that shrinks long enough eventually quits. The longer you wait, the fewer you keep.
P.P.S. The photo you take on day one matters more than anything on this page. Same part, same light, once a month. You won’t have to take anyone’s word for it, including mine.
What happens next
- Order today. It ships from our team, usually within a day.
- Two gummies with or without food. That’s the whole routine.
- The tracker and guides arrive with your order confirmation. Use the same-light photo trick.
- Ninety days is the checkpoint. Judge it there, not at three washes.
References
- Menopause (journal), 2022. Prevalence of female pattern hair loss in postmenopausal women: 52.2%.
- Newson, L. Poll of ~6,000 women: roughly half noticed hair thinning across the menopause transition. Approximately two in three women report hair changes during the transition.
- Maturitas, 2025. Estrogen and progesterone decline, relative androgen excess, and follicle miniaturization in the menopause transition.
- Reilly et al. (2024). Randomized, double-blind, placebo-controlled trial of a hydrolysed collagen (5 g) and vitamin C supplement: 27.6% increase in hairs per unit area versus placebo at 12 weeks. Dermatology Research and Practice.
- Patel et al. (2025). Double-blind RCT (n=105) of Bambusa arundinacea silica plus Sesbania grandiflora biotin: statistically significant reduction in hair fall and increased hair growth rate (~0.57 mm/day, silica + biotin arm) over 90 days. Cureus 17(7):e89118.
- Cho et al. (2014). Randomized, placebo-controlled trial of pumpkin seed oil in men (n=76), 24 weeks, including reported reduction in scalp DHT of approximately 40%. Evidence-Based Complementary and Alternative Medicine (PMC4017725). Ingredient-level research in men. It is not a women’s result and not a finished-product result.
- Methylsulfonylmethane (MSM) dose-response studies on hair and skin parameters (16-week and 120-day supplementation).
- Vitamin D3 and telogen effluvium; vitamin D receptor expression in hair follicles (PMC5007917).
- Mayo Clinic Proceedings, 2019. Kling JM et al. Cross-sectional survey of family medicine, internal medicine, and obstetrics and gynecology residents, 94(2):242-253: 12 of 177 (6.8%) reported feeling adequately prepared to manage menopause.
- Stuenkel CA, Santoro NF, Laughlin-Tommaso SK, Black A, Joffe H, Su HI. NAMS 2019 Pre-Meeting Symposium: The Perimenopause. Menopause (The Journal of The North American Menopause Society), 2020;27(7):735-745. PMID 32433263. Perimenopause per STRAW+10 spans the menopause transition plus the first year after the final menstrual period.
- Menopause. StatPearls [Internet], NCBI Bookshelf NBK507826. Perimenopause lasts an average of approximately 4 to 7 years and can extend considerably longer in some women.
This article is for informational purposes only and does not constitute medical advice. Talk to your doctor before starting any supplement, especially alongside prescription treatments. Individual results vary.
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.